Bones are very much alive and are constantly remodeling in response to the forces that are applied to them
Think of bone remodeling like repaving a road:
Cells go along and chew up the “old asphalt” (bone matrix)
Other cells follow behind them and lay down the “new asphalt”
As we age, the cells that lay down new bone slow down more than the ones that break down the old bone. This eventually leads to osteoporosis.
Remodeling is affected by other diseases, like diabetes, COPD or rheumatoid arthritis, and also by medications like steroids, chemotherapy or drugs that are used to block testosterone as part of prostate cancer treatments.
Smoking and alcohol consumption are also major inhibitors of bone metabolism! Stop smoking and limit alcohol to 2 drinks/day or less.
How do I know if I’m at risk for problems with my bones?
If the women in your family have had osteoporosis or broken hips
If you smoke, drink alcohol or have any inflammatory diseases like rheumatoid arthritis, ulcerative colitis, lupus, crohn’s disease, COPD, diabetes, or obesity.
If you have had problems with low vitamin D.
If you have lost height, changing posture or have nagging pain in your back.
If you have had certain types of non-traumatic fractures in the past.
If you have had to take steroids (prednisone) in high doses or for long periods of time.
If you had an early menopause or have a condition resulting in low testosterone.
If you have been critically ill and/or bedridden.
How do we find bone disorders?
The standard imaging is by a DEXA scan, which is like an X-ray but takes longer. We use a facility that also assesses the Trabecular Bone Score, or micro-architecture of the spine, as this can be a deciding factor about who needs treatment.
The scan produces a T-score reading, which compares your bone density to a young normal bone density.
A T-score between -1 to -2.5 is osteopenia, or early thinning.
A T-score worse than -2.5 is osteoporosis.
For young people, a Z-score worse than -2.0 is highly suggestive of osteoporosis.
Any non-traumatic fractures of the spine, low impact fractures of the hip/femur or a fracture around a new prosthetic implant also counts as osteoporosis.
How do we treat disorders of bone metabolism?
We always need to check to see if there are underlying causes for bone disorders and treat that (i.e., hyperthyroidism, lymphoma, multiple myeloma, overactive parathyroids, etc.)
Everyone should have adequate calcium and vitamin D in their diet or supplement, so the body has the right building blocks for healthy bone formation.
Because bones remodel in proportion to stress that’s applied to them, we recommend daily weight bearing exercise like you would do anyway for heart health.
We must avoid muscle wasting, or sarcopenia, and so diet should aim for protein intake of approximately 1.3g/kg daily.
We treat osteoporosis with drugs like Fosamax or Boniva. Their job is to slow down those cells that break down the old bone, so the “new asphalt-laying” cells can catch up. It takes months to years to see the effect.
There is another drug, Forteo, which boosts the activity of the cells that lay down new bone, and works to heal fractures quickly.
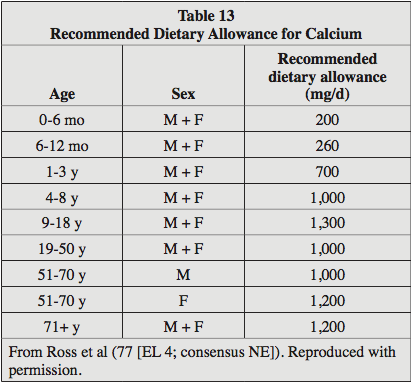
How much calcium and vitamin D do I need?
That depends on your age and your general bone health.
We want to maintain a blood vitamin D level between 30-40.
Getting calcium from the diet is best, but supplement if needed.
The average American diet contains 600mg of calcium daily, and each serving of dairy confers about another 150-300mg.
| Maximum Calcium Supplement: 600mg Take Calcium with Vitamin DTake Vitamin D with foodMaintain vitamin D level 30-40 |
How does obesity affect bones?
If you have a pair of identical twins, who both weigh 300 lbs, but one is a bodybuilder and one works at a desk all day. The body builder would have better bone density and health:
This is because his muscles are constantly pulling on his bones, applying stress, and the bones remodel in response.The other twin has a lot of weight on his bones, but less traction. This combined with the inflammatory state of obesity actually BLOCKS bone remodeling!
What medications are available?
Antiresorptives: Slow the breakdown of the old bone, so the new bone formation can catch up.
Fosamax (alendronate), Boniva (risedronate), Prolia (denosumab), Reclast (zoledronic acid), etc.
Anabolics: Work like a BIG boost to the cells that lay down new bone.
Forteo (Teriparatide), Tymlos (Abaloparatide)
Combination therapy: works mostly to boost the cells that lay down new bone, but also slows the breakdown of old bone
Evenity (Romosozumab)
What risks are associated with treatment?
Osteonecrosis of the jaw – (1 in 40,000)
Very rare at osteoporosis doses, and typically is only seen in the higher doses of drug that are used in cancer patients.
We screen everyone for risks (i.e., oral surgery, implants/extractions), and I have only VERY rarely seen this complication.
If you DO develop this complication, it usually can be managed with mouthwash, antibiotics and conservative management by an oral surgeon.
Atypical femur fractures – (1 in 20,000).
More likely to occur when a patient has taken the drug for more than 5 years.
Symptoms: nagging pain in the groin/upper thigh are hallmarks of these fractures.
Starting in year 3-5 we will re-evaluate your response to therapy and determine if a drug holiday is right for you, and this reduces the risk.
Osteosarcoma – (Tymlos & Forteo only)
If you have had radiation therapy to the spine, or when a patient is at risk for metastatic cancer, the risk outweighs the benefit of using these drugs.
Cardiovascular Disease – (Evenity only)
If you have had a heart attack, stent, bypass or stroke in the last year, this medication is not a good choice.
For any medication with anabolic effect, once you finish the course of treatment, you MUST follow it by taking an antiresorptive agent, or else we will LOSE the bone we built and we don’t get a “do-over.”
ResourcesNational Osteoporosis Foundation https://www.nof.org/patients/